
Opioid Misuse: A Review of the Main Issues, Challenges, and Strategies
 , , ,
, , ,  ,
,  , , , and
, , , and
Abstract
:1. Introduction and Background Literature
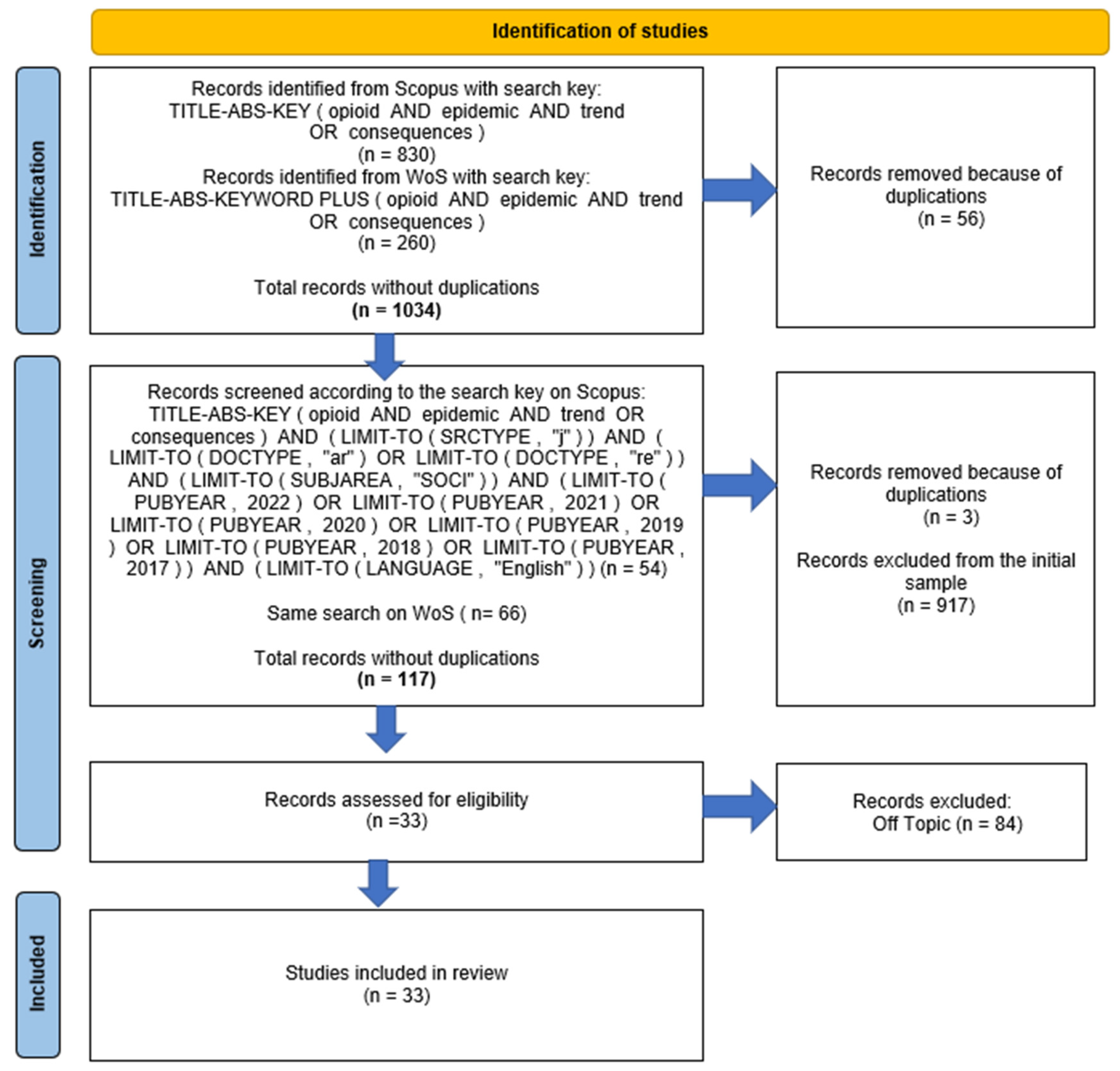
2. Methodology
Research question (RQ): What are the trends and consequences of opioid misuse analyzed in the recent literature?
3. Results
“I always said I would never do that [share needles]. (…) and then that’s when it happens. (…) This one time, I was in jail–I didn’t have anything, and I shot up in jail like an idiot. I didn’t know that everybody had hep C.”[54]
“(…) the results of this study can be used to inform counties considering implementing naloxone programs, an important medication used to reverse opiate overdose.”[12]
“I know that I personally do my best to monitor for signs of misuse or abuse and to counsel as necessary, but I don’t have access to patient charts, histories or diagnosis or to the attention of the patient as physicians do.”[53]
“(…) traditional utilization management approaches appeared to be ineffective in slowing the spread of the epidemic. We believed more could be done. We also recognized that no single entity could do this alone. We began working with many partners (…) coordinating teams internally, including our medical policy, pharmacy, and fraud teams, (…)”[5]
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Institute on Drug Abuse. Opioids. 2022. Available online: https://nida.nih.gov/drug-topics/opioids (accessed on 24 March 2022).
- Cuomo, A.; Cascella, M.; Forte, C.A.; Bimonte, S.; Esposito, G.; De Santis, S.; Cavanna, L.; Fusco, F.; Dauri, M.; Natoli, S.; et al. Careful Breakthrough Cancer Pain Treatment through Rapid-Onset Transmucosal Fentanyl Improves the Quality of Life in Cancer Patients: Results from the BEST Multicenter Study. J. Clin. Med. 2020, 9, 1003. [Google Scholar] [CrossRef] [PubMed]
- Centers for Desease Control and Prevention. Understanding the Epidemic. 2020. Available online: https://www.cdc.gov/drugoverdose/epidemic/index.html (accessed on 24 March 2022).
- Centers for Disease Control and Prevention NC for IP and C. Drug Overdose Deaths. 2021. Available online: https://www.cdc.gov/drugoverdose/deaths/index.html (accessed on 16 March 2022).
- DeShazer, C.; Dominic, O.; DeLeo, C.; Johnson, R. Impact of a Health System’s Three-Pronged Strategy to Address the Opioid Epidemic in DE, PA, and WV, 2013–2017. Open Public Health J. 2020, 13, 152–160. [Google Scholar] [CrossRef]
- Eeckhaut, M.C.W.; Wagner, J.; Neitzke-Spruill, L.; Walker, R.; Anderson, T.L. Is the gender gap in overdose deaths (still) decreasing? An examination of opioid deaths in Delaware, 2013–2017. J. Stud. Alcohol Drugs. 2020, 81, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Preventions. National Center, Control IP and Understanding the Epidemic; CDC: Atlanta, GA, USA, 2020. [Google Scholar]
- Rudd, R.A.; Paulozzi, L.J.; Bauer, M.J.; Burleson, R.W.; Carlson, R.E.; Dao, D.; Davis, D.W.; Dudek, J.; Eichler, B.A.; Fernandes, J.C.; et al. Increases in heroin overdose deaths—28 states, 2010 to 2012. Morb. Mortal Wkly. Rep. 2014, 63, 849. [Google Scholar]
- Gladden, R.M.; Martinez, P.; Seth, P. Fentanyl law enforcement submissions and increases in synthetic opioid–involved overdose deaths—27 states, 2013–2014. Morb. Mortal Wkly. Rep. 2016, 65, 837–843. [Google Scholar] [CrossRef]
- O’Donnell, J.K.; Halpin, J.; Mattson, C.L.; Goldberger, B.A.; Gladden, R.M. Deaths involving fentanyl, fentanyl analogs, and U-47,700—10 states, July–December 2016. MMWR Morb. Mortal Wkly. Rep. 2017, 66, 1197. [Google Scholar] [CrossRef]
- O’Donnell, J.K.; Gladden, R.M.; Seth, P. Trends in deaths involving heroin and synthetic opioids excluding methadone, and law enforcement drug product reports, by census region—United States, 2006–2015. Morb. Mortal Wkly. Rep. 2017, 66, 897. [Google Scholar] [CrossRef]
- Cordes, J. Spatial trends in opioid overdose mortality in North Carolina: 1999–2015. Southeast Geogr. 2018, 58, 193–211. [Google Scholar] [CrossRef]
- Graves, R.L.; Tufts, C.; Meisel, Z.F.; Polsky, D.; Ungar, L.; Merchant, R.M. Opioid discussion in the Twittersphere. Subst. Use Misuse 2018, 53, 2132–2139. [Google Scholar] [CrossRef]
- Chiu, A.S.; Healy, J.M.; DeWane, M.P.; Longo, W.E.; Yoo, P.S. Trainees as agents of change in the opioid epidemic: Optimizing the opioid prescription practices of surgical residents. J. Surg. Educ. 2018, 75, 65–71. [Google Scholar] [CrossRef]
- Cascella, M.; Monaco, F.; Nocerino, D.; Chinè, E.; Carpenedo, R.; Picerno, P.; Migliaccio, L.; Armignacco, A.; Franceschini, G.; Coluccia, S.; et al. Bibliometric Network Analysis on Rapid-Onset Opioids for Breakthrough Cancer Pain Treatment. J. Pain Symptom Manag. 2022, 63, 1041–1050. [Google Scholar] [CrossRef] [PubMed]
- El Moheb, M.; Mokhtari, A.; Han, K.; van Erp, I.; Kongkaewpaisan, N.; Jia, Z.; Rodriguez, G.; Kongwibulwut, M.; Kaafarani, H.M.; Sakran, J.V.; et al. Pain or No Pain, We Will Give You Opioids: Relationship Between Number of Opioid Pills Prescribed and Severity of Pain after Operation in US vs Non-US Patients. J. Am. Coll. Surg. 2020, 231, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Marinangeli, F.; Vittori, A.; Scala, C.; Piccinini, M.; Braga, A.; Miceli, L.; Vellucci, R. Open issues and practical suggestions for telemedicine in chronic pain. Int. J. Environ. Res. Public Health 2021, 18, 12416. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. Prescription Drug Use and Misuse in the United States: Results from the 2015 National Survey on Drug Use and Health; U.S. Department of Health & Human Services: Washington, DC, USA, 2016. Available online: https://www.samhsa.gov/data/report/prescription-drug-use-and-misuse-united-states-results-2015-national-survey-drug-use-and (accessed on 24 March 2022).
- Kaafarani, H.M.; Han, K.; El Moheb, M.; Kongkaewpaisan, N.; Jia, Z.; El Hechi, M.W.; van Wijck, S.; Breen, K.; Eid, A.; Rodriguez, G.; et al. Opioids After Surgery in the United States Versus the Rest of the World: The International Patterns of Opioid Prescribing (iPOP) Multicenter Study. Ann. Surg. 2020, 272, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Coben, J.H.; Davis, S.M.; Furbee, P.M.; Sikora, R.D.; Tillotson, R.D.; Bossarte, R.M. Hospitalizations for poisoning by prescription opioids, sedatives, and tranquilizers. Am. J. Prev. Med. 2010, 38, 517–524. [Google Scholar] [CrossRef]
- Strassels, S.A. Economic burden of prescription opioid misuse and abuse. J. Manag. Care Pharm. 2009, 15, 556–562. [Google Scholar] [CrossRef]
- El Moheb, M.; Herrera-Escobar, J.P.; Breen, K.; Orlas, C.; Haynes, A.N.; Levy-Carrick, N.C.; Nehra, D.; Sanchez, S.E.; Salim, A.; Velmahos, G.; et al. Long-term outcomes of psychoactive drug use in trauma patients: A multicenter patient-reported outcomes study. J. Trauma Acute Care Surg. 2021, 90, 319–324. [Google Scholar] [CrossRef]
- Miceli, L.; Bednarova, R.; Santori, E.; Spizzichino, M.; Botti, R.; Casciello, M.; Della Rocca, G. Outpatient therapeutic chronic opioid consumption in Italy: A one-year survey. Minerva Anestesiol. 2017, 83, 33–40. [Google Scholar] [CrossRef]
- Miceli, L.; Bednarova, R.; Rizzardo, A.; Cuomo, A.; Cascella, M.; Riccardi, I.; Vetrugno, L.; Bove, T. Opioids prescriptions in pain therapy and risk of addiction: A one-year survey in Italy Analysis of national opioids database. Ann. Ist. Super. Sanita. 2018, 54, 370–374. [Google Scholar]
- Miceli, L.; Bednarova, R.; Cuomo, A.; Cascella, M.; Guardamagna, V.; Romualdi, P.; Marinangeli, F. Prescribing opioids to patients with chronic pain: Translation of the opioid risk tool into Italian. Minerva Anestesiol. 2020, 86, 693–695. [Google Scholar] [CrossRef]
- Manchikanti, L.; Fellows, S.H.B.; Janata, J.W.; Pampati, V.; Grider, J.S.; Boswell, M.V. Opioid epidemic in the United States. Pain Physician 2012, 15 (Suppl. S3), ES9–ES38. [Google Scholar] [CrossRef] [PubMed]
- Massaro, M.; Dumay, J.C.; Guthrie, J. On the shoulders of giants: Undertaking a structured literature review in accounting. Account. Audit. Acc. J. 2016, 29, 767–901. [Google Scholar] [CrossRef]
- Palumbo, R. Contextualizing co-production of health care: A systematic literature review. Int. J. Public Sect. Manag. 2016, 29, 72–90. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar]
- Vivolo-Kantor, A.M.; Seth, P.; Gladden, R.M.; Mattson, C.L.; Baldwin, G.T.; Kite-Powell, A.; Coletta, M.A. Vital signs: Trends in emergency department visits for suspected opioid overdoses—United States, July 2016–September 2017. Morb. Mortal Wkly. Rep. 2018, 67, 279. [Google Scholar] [CrossRef]
- Fleischauer, A.T.; Ruhl, L.; Rhea, S.; Barnes, E. Hospitalizations for endocarditis and associated health care costs among persons with diagnosed drug dependence—North Carolina, 2010–2015. MMWR Morb. Mortal Wkly. Rep. 2017, 66, 569. [Google Scholar] [CrossRef]
- Guy, G.P., Jr.; Haegerich, T.M.; Evans, M.E.; Losby, J.L.; Young, R.; Jones, C.M. Vital signs: Pharmacy-based naloxone dispensing—United States, 2012–2018. Morb. Mortal Wkly. Rep. 2019, 68, 679. [Google Scholar] [CrossRef]
- Lynch, S.; Sherman, L.; Snyder, S.M.; Mattson, M. Trends in infants reported to child welfare with neonatal abstinence syndrome (NAS). Child Youth Serv. Rev. 2018, 86, 135–141. [Google Scholar] [CrossRef]
- Strickler, G.K.; Kreiner, P.W.; Halpin, J.F.; Doyle, E.; Paulozzi, L.J. Opioid prescribing behaviors—prescription behavior surveillance system, 11 states, 2010–2016. MMWR Surveill. Summ. 2020, 69, 1–14. [Google Scholar] [CrossRef]
- Saunders, J.B.; Jarlenski, M.P.; Levy, R.; Kozhimannil, K.B. Federal and state policy efforts to address maternal opioid misuse: Gaps and challenges. Women’s Health Issues 2018, 28, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Daniulaityte, R.; Silverstein, S.M.; Crawford, T.N.; Martins, S.S.; Zule, W.; Zaragoza, A.J.; Carlson, R.G. Methamphetamine use and its correlates among individuals with opioid use disorder in a Midwestern US city. Subst. Use Misuse 2020, 55, 1781–1789. [Google Scholar] [CrossRef] [PubMed]
- Chiarello, E. Where movements matter: Examining unintended consequences of the pain management movement in medical, criminal justice, and public health fields. Law Policy 2018, 40, 79–109. [Google Scholar] [CrossRef]
- Seltzer, N. The economic underpinnings of the drug epidemic. SSM Popul. Health 2020, 12, 100679. [Google Scholar] [CrossRef]
- Bushman, G.; Victor, B.G.; Ryan, J.P.; Perron, B.E. In utero exposure to opioids: An observational study of mothers involved in the child welfare system. Subst. Use Misuse 2018, 53, 844–851. [Google Scholar] [CrossRef]
- Sud, A.; Doukas, K.; Hodgson, K.; Hsu, J.; Miatello, A.; Moineddin, R.; Paton, M. A retrospective quantitative implementation evaluation of Safer Opioid Prescribing, a Canadian continuing education program. BMC Med. Educ. 2021, 21, 101. [Google Scholar] [CrossRef]
- Queeneth, U.; Bhimanadham, N.N.; Mainali, P.; Onyeaka, H.K.; Pankaj, A.; Patel, R.S. Heroin overdose-related child and adolescent hospitalizations: Insight on comorbid psychiatric and substance use disorders. Behav. Sci. 2019, 9, 77. [Google Scholar] [CrossRef]
- Feinglass, J.; Wang, J.A.; Ye, J.; Tessier, R.; Kim, H. Hospital Care for Opioid use in Illinois, 2016–2019. J. Behav. Health Serv. Res. 2021, 48, 597–609. [Google Scholar] [CrossRef]
- Sobotka, T.C.; Stewart, S.A. Stereotyping and the opioid epidemic: A conjoint analysis. Soc. Sci. Med. 2020, 255, 113018. [Google Scholar] [CrossRef]
- Aguilar-Amaya, M.; Gutiérrez, M. Implementing compassion fatigue prevention for lay employees conducting naloxone training: An example from rural Arizona. J. Soc. Work Pract. Addict. 2019, 19, 314–321. [Google Scholar] [CrossRef]
- Wagner, J.; Neitzke-Spruill, L.; Donnelly, E.A.; O’Connell, D.J.; Anderson, T.L. The Current Community Context of Overdose Deaths: Relations among Drug Types, Drug Markets, and Socioeconomic Neighborhood Characteristics 1. In Sociological Forum; Wiley Online Library: New York, NY, USA, 2021; pp. 1005–1027. [Google Scholar]
- Wentzlof, C.A.; Boman, J.H., IV; Pryor, C.; Hemez, P. Kicking the can down the street: Social policy, intimate partner violence, and homicide during the opioid crisis. Subst. Use Misuse 2021, 56, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Gollust, S.E.; Haselswerdt, J. A crisis in my community? Local-level awareness of the opioid epidemic and political consequences. Soc. Sci. Med. 2021, 291, 114497. [Google Scholar] [CrossRef]
- Odusola, F.; Kaufman, J.; Turrigiano, E.; Aydinoglo, N.; Shulman, M.; Kidd, J.; Hu, M.C.; Levin, F.R. Predoctoral substance use disorders curricula: A survey analysis and experiential pedagogy. J. Dent. Educ. 2021, 85, 1664–1673. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.; Roth, R.; Wallman, J. Homicide and the Opioid Epidemic: A Longitudinal Analysis. Homicide Stud. 2021, 10887679211054418. [Google Scholar] [CrossRef]
- Testa, A.; Weiss, D.B.; Santos, M.R. Opioid mortality, public health care expenditures, and cross-national homicide rates: Findings from 25 OECD countries, 2000–2017. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 57, 673–682. [Google Scholar] [CrossRef] [PubMed]
- Sud, A.; Hodgson, K.; Bloch, G.; Upshur, R. A Conceptual Framework for Continuing Medical Education and Population Health. Teach. Learn Med. 2021; in press. [Google Scholar] [CrossRef]
- Rao, D.; Giannetti, V.; Kamal, K.M.; Covvey, J.R.; Tomko, J.R. Pharmacist Views Regarding the Prescription Opioid Epidemic. Subst. Use Misuse 2021, 56, 2096–2105. [Google Scholar] [CrossRef]
- Scorsone, K.L.; Haozous, E.A.; Hayes, L.; Cox, K.J. Ending the Chase: Experiences of Rural Individuals with Opioid Use Disorder. Subst. Use Misuse 2021, 56, 1224–1231. [Google Scholar] [CrossRef]
- Cashwell, S.T.; Campbell, M.; Cowser, J. Stone soup: Social work community engagement in rural America’s opioid crisis. Soc. Work Ment. Health 2021, 19, 81–87. [Google Scholar] [CrossRef]
- Cotti, C.D.; Gordanier, J.M.; Ozturk, O.D. The relationship of opioid prescriptions and the educational performance of children. Soc. Sci. Med. 2020, 265, 113406. [Google Scholar] [CrossRef]
- Barnes, M.C.; Kelly, T.J.; Piemonte, C.M. Demanding Better: A Case for Increased Funding and Involvement of State Medical Boards in Response to America’s Drug Abuse Crisis. J. Med. Regul. 2020, 106, 6–21. [Google Scholar] [CrossRef]
- Ho, J.A.; Rovzar, A.O. Preventing Neonatal Abstinence Syndrome within the Opioid Epidemic: A Uniform Facilitative Policy. Harv. J. Legis. 2017, 54, 423. [Google Scholar]
- Massaro, M.; Dumay, J.; Garlatti, A. Public sector knowledge management: A structured literature review. J. Knowl. Manag. 2015, 19, 530–558. [Google Scholar] [CrossRef]
- Guthrie, J.; Dumay, J.; Puntillo, P. IC and public sector: A structured literature review. J. Intellect. Cap. 2015, 16, 267–284. [Google Scholar]
- Dal Mas, F.; Massaro, M.; Lombardi, R.; Garlatti, A. From Output to Outcome Measures in the Public Sector. A Structured Literature Review. Int. J. Organ. Anal. 2019, 27, 1631–1656. [Google Scholar] [CrossRef]
- Dal Mas, F.; Garcia-Perez, A.; Sousa, M.J.; Lopes da Costa, R.; Cobianchi, L. Knowledge Translation in the Healthcare Sector. A Structured Literature Review. Electron J. Knowl. Manag. 2020, 18, 198–211. [Google Scholar] [CrossRef]
- Bert, F.; Galis, V.; Passi, S.; Rosaria Gualano, M.; Siliquini, R. Differences existing between USA and Europe in opioids purchase on Internet: An interpretative review. J. Subst. Use 2015, 20, 200–207. [Google Scholar] [CrossRef]
- Angelos, P. Interventions to Improve Informed Consent: Perhaps Surgeons Should Speak Less and Listen More. JAMA Surg. 2020, 155, 13–14. [Google Scholar] [CrossRef]
- Lamplot, J.D.; Premkumar, A.; James, E.W.; Lawton, C.D.; Pearle, A.D. Postoperative Disposal of Unused Opioids: A Systematic Review. HSS J. 2021, 17, 235–243. [Google Scholar] [CrossRef]
- Kaafarani, H.M.A.; Eid, A.I.; Antonelli, D.M.; Chang, D.C.; Elsharkawy, A.E.; Elahad, J.A.; Lancaster, E.A.; Schulz, J.T.; Melnitchouk, S.I.; Kastrinakis, W.V.; et al. Description and Impact of a Comprehensive Multispecialty Multidisciplinary Intervention to Decrease Opioid Prescribing in Surgery. Ann. Surg. 2019, 270, 452–462. [Google Scholar] [CrossRef]
- Kaafarani, H.M.A.; Weil, E.; Wakeman, S.; Ring, D. The Opioid Epidemic and New Legislation in Massachusetts: Time For a Culture Change in Surgery? Ann. Surg. 2017, 265, 731–733. [Google Scholar] [CrossRef]
- Ling, W.; Mooney, L.; Hillhouse, M. Prescription opioid abuse, pain and addiction: Clinical issues and implications. Drug Alcohol Rev. 2011, 30, 300–305. [Google Scholar] [CrossRef]
- Bongiorno, G.; Biancuzzi, H.; Dal Mas, F.; Bednarova, R.; Miceli, L. The Rehabilitation Tailor: Applying personalized medicine to cancer recovery. Front. Glob. Women’s Health 2022, 3, 914302. [Google Scholar] [CrossRef] [PubMed]
- Ung, A.; Salamonson, Y.; Hu, W.; Gallego, G. Assessing knowledge, perceptions and attitudes to pain management among medical and nursing students: A review of the literature. Br. J. Pain 2015, 10, 8–21. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.S.; Stein, A.; Thomas, H.; Kaur, H. The use of Electronic Health Records to Support Population Health: A Systematic Review of the Literature. J. Med. Syst. 2018, 42, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, E.M. Diffusion of Innovations, 5th ed.; Free Press Simon and Schuster: New York, NY, USA, 2003; pp. 1–576. [Google Scholar]
- Green, L.W.; Gielen, A.C.; Ottoson, J.M.; Peterson, D.V.; Kreuter, M.W. Health Program Planning, Implementation, and Evaluation Creating Behavioral, Environmental, and Policy Change; Johns Hopkings University Press: Baltimore, MD, USA, 2022. [Google Scholar]
- Green, L.W.; Kreuter, M.W. CDC’s Planned Approach to Community Health as an Application of PRECEED and an Inspiration for PROCEED. J. Health Educ. 1992, 23, 140–147. [Google Scholar] [CrossRef]
- CDC Centers for Disease Control and Prevention. CDC’s Response to the Opioid Overdose Epidemic; CDC: Atlanta, GA, USA, 2019. [Google Scholar]


{kind=link}
| N. | Authors | Title | Journal | Reference |
|---|---|---|---|---|
| 1 | Vivolo-Kantor A.M., Seth P., Gladden R.M., Mattson C.L., Baldwin G.T., Kite-Powell A., Coletta M.A. | Vital signs: Trends in emergency department visits for suspected opioid overdoses—United States, July 2016–September 2017 | Morbidity and Mortality Weekly Report | [31] |
| 2 | Fleischauer A.T., Ruhl L., Rhea S., Barnes E. | Hospitalizations for endocarditis and associated health care costs among persons with diagnosed drug dependence-North Carolina, 2010–2015 | Morbidity and Mortality Weekly Report | [32] |
| 3 | Chiu A.S., Healy J.M., DeWane M.P., Longo W.E., Yoo P.S. | Trainees as Agents of Change in the Opioid Epidemic: Optimizing the Opioid Prescription Practices of Surgical Residents | Journal of Surgical Education | [14] |
| 4 | Guy G.P., Jr., Haegerich T.M., Evans M.E., Losby J.L., Young R., Jones C.M. | Vital signs: Pharmacy-based naloxone dispensing—United States, 2012–2018 | Morbidity and Mortality Weekly Report | [33] |
| 5 | Lynch S., Sherman L., Snyder S.M., Mattson M. | Trends in infants reported to child welfare with neonatal abstinence syndrome (NAS) | Children and Youth Services Review | [34] |
| 6 | Strickler G.K., Kreiner P.W., Halpin J.F., Doyle E., Paulozzi L.J. | Opioid prescribing behaviors-Prescription behavior surveillance system, 11 states, 2010–2016 | MMWR Surveillance Summaries | [35] |
| 7 | Graves R.L., Tufts C., Meisel Z.F., Polsky D., Ungar L., Merchant R.M. | Opioid Discussion in the Twittersphere | Substance Use and Misuse | [13] |
| 8 | Saunders J.B., Jarlenski M.P., Levy R., Kozhimannil K.B. | Federal and State Policy Efforts to Address Maternal Opioid Misuse: Gaps and Challenges | Women’s Health Issues | [36] |
| 9 | Daniulaityte R., Silverstein S.M., Crawford T.N., Martins S.S., Zule W., Zaragoza A.J., Carlson R.G. | Methamphetamine Use and Its Correlates among Individuals with Opioid Use Disorder in a Midwestern U.S. City | Substance Use and Misuse | [37] |
| 10 | Eeckhaut M.C.W., Wagner J., Neitzke-Spruill L., Walker R., Anderson T.L. | Is the gender gap in overdose deaths (Still) decreasing? an examination of opioid deaths in Delaware, 2013–2017 | Journal of Studies on Alcohol and Drugs | [6] |
| 11 | Cordes J. | Spatial trends in opioid overdose mortality in North Carolina: 1999–2015 | Southeastern Geographer | [12] |
| 12 | Chiarello E. | Where Movements Matter: Examining Unintended Consequences of the Pain Management Movement in Medical, Criminal Justice, and Public Health Fields | Law and Policy | [38] |
| 13 | Seltzer N. | The economic underpinnings of the drug epidemic | SSM-Population Health | [39] |
| 14 | Bushman G., Victor B.G., Ryan J.P., Perron B.E. | In Utero Exposure to Opioids: An Observational Study of Mothers Involved in the Child Welfare System | Substance Use and Misuse | [40] |
| 15 | Sud A., Doukas K., Hodgson K., Hsu J., Miatello A., Moineddin R., Paton M. | A retrospective quantitative implementation evaluation of Safer Opioid Prescribing, a Canadian continuing education program | BMC Medical Education | [41] |
| 16 | Queeneth U., Bhimanadham N.N., Mainali P., Onyeaka H.K., Pankaj A., Patel R.S. | Heroin overdose-related child and adolescent hospitalizations: Insight on comorbid psychiatric and substance use disorders | Behavioral Sciences | [42] |
| 17 | Feinglass J., Wang J.A., Ye J., Tessier R., Kim H. | Hospital Care for Opioid use in Illinois, 2016–2019 | Journal of Behavioral Health Services and Research | [43] |
| 18 | Sobotka T.C., Stewart S.A. | Stereotyping and the opioid epidemic: A conjoint analysis | Social Science and Medicine | [44] |
| 19 | Aguilar-Amaya M., Gutiérrez M., Sr. | Implementing Compassion Fatigue Prevention for Lay Employees Conducting Naloxone Training: An Example from Rural Arizona | Journal of Social Work Practice in the Addictions | [45] |
| 20 | Wagner J., Neitzke-Spruill L., Donnelly E.A., O’Connell D.J., Anderson T.L. | The Current Community Context of Overdose Deaths: Relations among Drug Types, Drug Markets, and Socioeconomic Neighborhood Characteristics | Sociological Forum | [46] |
| 21 | Wentzlof C.A., Boman IV J.H., Pryor C., Hemez P. | “Kicking the Can down the Street”: Social Policy, Intimate Partner Violence, and Homicide during the Opioid Crisis | Substance Use and Misuse | [47] |
| 22 | Gollust S.E., Haselswerdt J. | A crisis in my community? Local-level awareness of the opioid epidemic and political consequences | Social Science and Medicine | [48] |
| 23 | Odusola F., Kaufman J., Turrigiano E., Aydinoglo N., Shulman M., Kidd J., Hu M.-C., Levin F.R. | Predoctoral substance use disorders curricula: A survey analysis and experiential pedagogy | Journal of Dental Education | [49] |
| 24 | Rosenfeld R., Roth R., Wallman J. | Homicide and the Opioid Epidemic: A Longitudinal Analysis | Homicide Studies | [50] |
| 25 | Testa A., Weiss D.B., Santos M.R. | Opioid mortality, public health care expenditures, and cross-national homicide rates: findings from 25 OECD countries, 2000–2017 | Social Psychiatry and Psychiatric Epidemiology | [51] |
| 26 | Sud A., Hodgson K., Bloch G., Upshur R. | A Conceptual Framework for Continuing Medical Education and Population Health | Teaching and Learning in Medicine | [52] |
| 27 | Rao D., Giannetti V., Kamal K.M., Covvey J.R., Tomko J.R. | Pharmacist Views Regarding the Prescription Opioid Epidemic | Substance Use and Misuse | [53] |
| 28 | Scorsone K.L., Haozous E.A., Hayes L., Cox K.J. | Ending the Chase: Experiences of Rural Individuals with Opioid Use Disorder | Substance Use and Misuse | [54] |
| 29 | Cashwell S.T., Campbell M., Cowser J. | Stone soup: social work community engagement in rural America’s opioid crisis | Social Work in Mental Health | [55] |
| 30 | Cotti C.D., Gordanier J.M., Ozturk O.D. | The relationship of opioid prescriptions and the educational performance of children | Social Science and Medicine | [56] |
| 31 | Barnes M.C., Kelly T.J., Piemonte C.M. | Demanding Better: A Case for Increased Funding and Involvement of State Medical Boards in Response to America’s Drug Abuse Crisis | Journal of Medical Regulation | [57] |
| 32 | Deshazer C., Dominic O., Deleo C., Johnson R. | Impact of a health system’s three-pronged strategy to address the opioid epidemic in de, pa, and wv, 2013–2017 | Open Public Health Journal | [5] |
| 33 | Ho J.A., Rovzar A.O. | Preventing neonatal abstinence syndrome within the opioid epidemic: A uniform facilitative policy | Harvard Journal on Legislation | [58] |
| Node | Number of Coding | |
|---|---|---|
| 01_Authors 01_Academics 02_Not academics/Practitioners 03_Collaboration between academics and practitioners | 19 5 9 | 33 |
| 02_Geographic area 01_United States 02_Not localized 03_Canada 04_Multi-area | 28 3 1 1 | 33 |
| 03_Type of pathology/department of reference 01_In global terms 02_Chronic pain 03_Emergency 04_Cardiology 05_Post operative pain 06_Neonatology/Pediatrics 07_Twin epidemic | 19 1 3 1 1 5 8 | 33 |
| 04_Research method 01_Qualitative 02_Quantitative 01_Interview 01_Other 03_Literature Review | 6 5 20 2 | 33 |
| 05_Type of impact 01_Social 01_Increase in deaths 02_Abuse of minors 03_Illegal use of methamphetamine, fentanyl, ecc. 04_Domestic violence 05_Homicide 06_Negative repercussions on academic performance 02_Economic 01_Increase in Medicaid enrollments 02_Increase in healthcare costs 03_Public health 01_Increase in ER accesses 02_Infectious Complications 03_Endiocarditis 04_Increase in the use of naloxone 05_Nonatal abstinence syndrome 06_Preterm birth 07_Sleep issues 04_Politics and justice 05_Professional training | 24 1 9 2 3 1 1 8 2 2 1 1 2 1 1 13 1 | 33 |
| 06_Stakeholders 01_Patients 02_Health system/Pharmacists 03_Contributions 04_Minors 05_Childcare system 06_Justice 07_Families 08_Administrative employees 09_Communities 10_Schools 11_Financers 12_Social assistants 13_State Medical Commission | 16 14 2 5 3 15 6 1 3 1 1 1 1 | |
| 07_Recommended strategies 01_Yes 01_Prevention enhancement 02_Medical assistance 03_Real-time data to deal with overdoses 04_Real-time data to manage outbreaks 05_Increase/improve naloxone prescriptions 06_Increase training 07_Syringe Service Programs 08_Opioid treatment programs 09_Involvement of political decision makers 10_More personalized care 11_Training of patients and families 12_Strengthening the collaboration between the health and safety sector 13_Improvement of childcare services 14_New best practices 15_Research/Financing 16_Multi-sector approaches 17_Wage increases 18_Increase in employment 19_Reduction in stereotypes 20_Increase access to health care 21_Reduction in over-policing 22_More investments in public health 23_Reduction in barriers 24_ Legalization of marijuana 25_Improve the relationship between pharmacist and general practitioner 26_Involvement of social workers 27_Better health check on possible opioid problems 28_Increase in the fight against drug dealing 02_No | 8 5 3 5 5 11 2 6 3 3 4 1 1 3 6 5 1 1 1 1 2 3 1 1 1 1 2 3 0 | |
| Type of Impact | Most Relevant Subgroups | References | Extracted Contents |
|---|---|---|---|
| Social, Health and Public Health | 1. Illegal use of methamphetamine-fentanyl-etc. | Eeckhaut, M.C.W., et al. 2020 [6] | “Synthetic opioids are now driving the US epidemic11 as prescription opioid is being replaced by heroin adulterated with fentanyl and its analogues.” “…prescription opioids are a “gateway” to other more dangerous or illegal opioids (e.g., heroin, illicitly manufactured fentanyl)…” |
| 2. Homicides | Rosenfeld, R., et al., 2020 [50] Testa, A., et al., 2021 [51] | “The results reveal a positive association between change over time in homicide and opioid-related deaths, net of multiple socioeconomic and demographic controls, in both the Non-Hispanic White and Black population.” “Study findings revealed a positive bivariate association between opioid mortality and homicide rates.” | |
| 3. Increase in the number of deaths | Chiu, A.S., et al., 2018 [14] U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2020 Seltzer, N., 2020 [39] | “As of 2014, the number of opioid-related deaths in the United States had risen to nearly 50,000 a year, a number now greater than the annual deaths from motor vehicle accidents.” “In 2017, a total of 70,237 persons in the United States died from a drug overdose, and 67.8% of these deaths involved an opioid recognized as a controlled/scheduled substance by the federal government.” Drug overdose deaths in the United States continued to rise (…) reducing overall life expectancy (…) trend in life expectancy that has not occurred in over a century.” | |
| Medical | 1. Infectious complications | U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2017 | “(…) infectious complications of intravenous drug use constitute a major cause of morbidity leading to hospitalization” |
| 2. Neonatal abstinence syndrome | Saunders, J.B., et al., 2018 [36] | “Opioid misuse during pregnancy is increasingly common and is associated with preterm birth and neonatal abstinence syndrome.” | |
| Economic, politics and justice | 1. Increase in health care costs | DeShazer, C., et al., 2020 [5] Ho, J.A., et al., 2017 [58] | “Employees with substance abuse disorder have three times more in health care costs of the average worker.” “The expenses of treating, monitoring, and rehabilitating these chemically dependent newborns are predominantly shouldered by state taxpayers and are extremely costly, with a mean cost per stay exceeding $90,000 for pharmacologically treated cases.” |
| 2. Violence and safety | Testa, A., et al., 2021 [51] Gollust, S.E., et al. 2021 [48] Saunders, J.B., et al., 2018 [36] | “The pharmacological effects of opioids may prompt users to become involved in illicit markets and the violence associated with such markets (…) Individuals who are physically dependent on opioids may also resort to economic-compulsive offending, which may include violence in the instance of robbery or drug dealing, to support their use.” “The opioid epidemic has had a profound effect on American public health, and studies suggest it has had a profound effect on American politics as well. Research suggests a relationship between the severity of the opioid crisis in a community and aggregate-level political behavior, including voting for Donald Trump in 2016 (…)” “State policymakers have made broad efforts to address the opioid epidemic at the public health and safety level (e.g., prescription drug monitoring programs) and the health care system level (…). Legislatures, governors, and state agencies have also taken specific steps to combat increasing trends in opioid misuse among pregnant women.” |
| Stakeholders | References | Extracted Contents |
|---|---|---|
| Patients | Chiu, A.S., et al., 2018 [14] Saunders, J.B., et al., 2018 [36] Seltzer, N., 2020 [39] Scorsone, K.L., et al., 2021 [54] | “(…) excess prescription of opioids present a hazard to both the patient and those around them.” “Strategies to address opioid misuse before pregnancy are efforts for the general population that also happen to include reproductive-age women.” “The drug epidemic continues to disrupt the lives of individuals, families, and communities throughout the country.” “That’s not how it works. You’re doing it because you have to because your body is telling you that you need it. Once you get that chemical imbalance in your brain, that’s it. You will always be an addict.” |
| Justice | Scorsone, K.L., et al., 2021 [54] Wagner, J., et al., 2021 [46] | “All of the participants described having lost employment income, leading to reliance on stealing from family and burglary.” “I broke into one house, and I got caught for it, because I was sloppy about it, but I admitted to it when the cops showed up, and I knew the people. I told them, “Yeah, I’m an addict. I needed to get my fix.” “(economic) disadvantage is a highly significant predictor of increased drug selling and drug possession arrests in a neighborhood (…). Drug possession arrests, in turn, are associated with higher neighborhood opioid overdose death rates (…).” |
| Healthcare System/Pharmacists | Rao, D., et al., 2021 [53] | “Oftentimes, pharmacists call prescribers and question long term use of medications and are met with trouble.” “Declining to fill a prescription based on clinical judgment (in absence of obvious red flags like early fills) is an uncomfortable concept for many pharmacists, I feel, because there is concern that it will damage patient and physician relationships by making you the “difficult” or “intrusive” pharmacist. |
| Families | Wentzlof, C.A., et al., 2021 [47] | “Research has established a strong, positive correlation between homicides and substance use and also between homicides and intimate partner violence.” |
| Minors | Queeneth, U., et al., 2019 [42] Lynch, S., et al., 2018 [34] | “Younger children are more vulnerable to the accidental ingestion of opioids. Certain strategies should be developed and also implemented to curb heroin overdoses in the pediatric population.” “In the past 18 years, nearly 8986 children and adolescents have died from illicit opioid use (…)” “The recent opioid epidemic has led to rising numbers of women who use opioids during pregnancy and infants born with neonatal abstinence syndrome (NAS), raising the question of whether there has been a consequent rise in the numbers of these infants reported to the child welfare system.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biancuzzi, H.; Dal Mas, F.; Brescia, V.; Campostrini, S.; Cascella, M.; Cuomo, A.; Cobianchi, L.; Dorken-Gallastegi, A.; Gebran, A.; Kaafarani, H.M.; et al. Opioid Misuse: A Review of the Main Issues, Challenges, and Strategies. Int. J. Environ. Res. Public Health 2022, 19, 11754. https://doi.org/10.3390/ijerph191811754
Biancuzzi H, Dal Mas F, Brescia V, Campostrini S, Cascella M, Cuomo A, Cobianchi L, Dorken-Gallastegi A, Gebran A, Kaafarani HM, et al. Opioid Misuse: A Review of the Main Issues, Challenges, and Strategies. International Journal of Environmental Research and Public Health. 2022; 19(18):11754. https://doi.org/10.3390/ijerph191811754
Chicago/Turabian StyleBiancuzzi, Helena, Francesca Dal Mas, Valerio Brescia, Stefano Campostrini, Marco Cascella, Arturo Cuomo, Lorenzo Cobianchi, Ander Dorken-Gallastegi, Anthony Gebran, Haytham M. Kaafarani, and et al. 2022. "Opioid Misuse: A Review of the Main Issues, Challenges, and Strategies" International Journal of Environmental Research and Public Health 19, no. 18: 11754. https://doi.org/10.3390/ijerph191811754